Chronic Pancreatitis
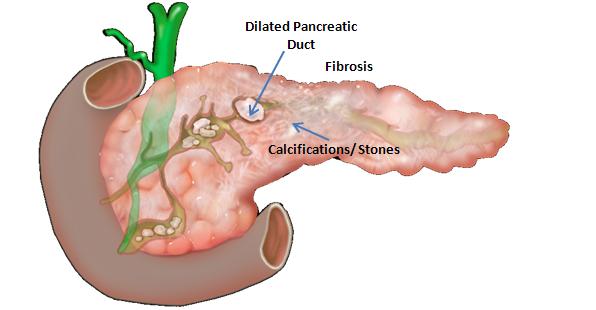
Chronic pancreatitis is a syndrome defined by chronic, progressive pancreatic inflammation, fibrosis, and scarring, resulting in damage to and loss of exocrine (acinar), endocrine (islet cells), and ductal cells. The syndrome is commonly associated with clinical features of abdominal pain, exocrine and endocrine insufficiency, secondary pancreatic cancer, and other complications.
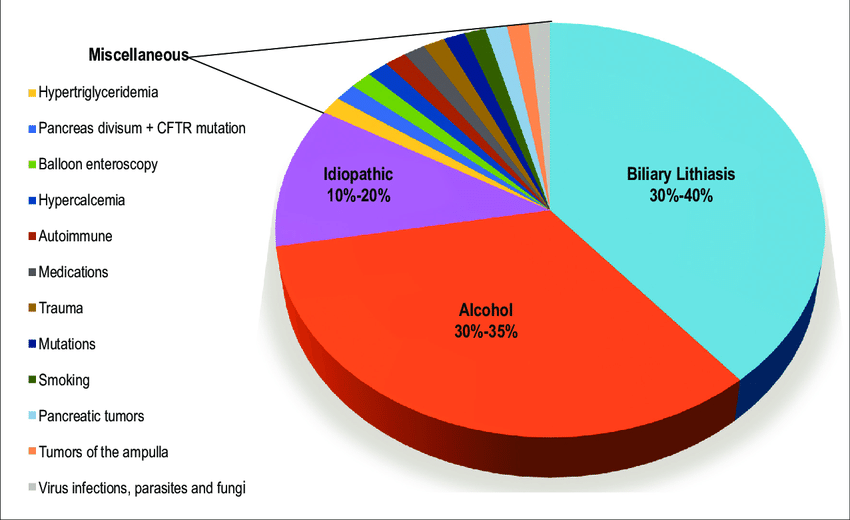
The most common cause of chronic pancreatitis is long-term alcohol abuse – it is thought to account for between 70 to 80 percent of all cases. Other causes include hereditary (PRSS1, SPINK1, CFTR, CTRC, CASR genetic variations), autoimmune, anatomic (pancreas divisum), obstructive, hyperlipidemia and idiopathic.
Pancreatic exocrine insufficiency (PEI), characterized by inadequate pancreatic secretion of digestive enzymes and bicarbonate, is one of the most significant complications of CP, affecting >50% of diagnosed patients. It manifests as steatorrhea (often without diarrhea), weight loss, malnutrition, metabolic bone disease, and vitamin and mineral deficiency. Symptomatic PEI does not occur until approximately 90% of pancreatic exocrine function is lost.
More than half of all patients with CP develop diabetes due to the loss of complete islet cell mass; this is sometimes referred to as Pancreatogenic diabetes or type 3c diabetes. It puts patients at a particularly high risk of developing secondary pancreatic carcinoma.
Current management of CP involves alcohol and tobacco abstinence, a multidisciplinary team approach to pain management, medical treatment of PEI, addressing malnutrition and osteoporosis, and adjustment of pancreatic exocrine replacement agents (PERT) and diabetic agents.
Severe chronic pain sometimes does not respond to painkilling medications. Following are the different forms of surgery that may be indicated in those severe cases:
Endoscopic management : Pancreatic ductal stone removal for intractable pain
Pancreatic resection : The head of the pancreas is surgically removed. This not only relieves the pain caused by inflammation irritating the nerve endings, but it also reduces pressure on the ducts. Three main techniques are used for pancreas resection:
![]() Beger procedure
Beger procedure
![]() Frey Procedure
Frey Procedure
![]() Pylorus preserving pancreaticoduodenectomy (PPPD)
Pylorus preserving pancreaticoduodenectomy (PPPD)
Total Pancreatectomy : This involves the surgical removal of the whole pancreas. It is very effective in dealing with severe pain. However, due to complete loss of exocrine and endocrine functions after total pancreatectomy; it is usually followed by pancreas transplant (PT) or autologous pancreatic islet cell transplantation (APICT)